




Along with the need to drink fresh water, which humans can normally attain in all except the most extreme situations, the need for food is the most fundamental and important human need.
More than 1 in 10 U.S. households contain people who live without enough nourishing food, and this lack of proper nourishment has profound effects on their abilities to create effective lives (Hunger Notes, n.d.). 1When people are extremely hungry, their motivation to attain food completely changes their behavior. Hungry people become listless and apathetic to save energy and then become completely obsessed with food. Ancel Keys and his colleagues (Keys, Brožek, Henschel, Mickelsen, & Taylor, 1950) 2 found that volunteers who were placed on severely reduced-calorie diets lost all interest in sex and social activities, becoming preoccupied with food.
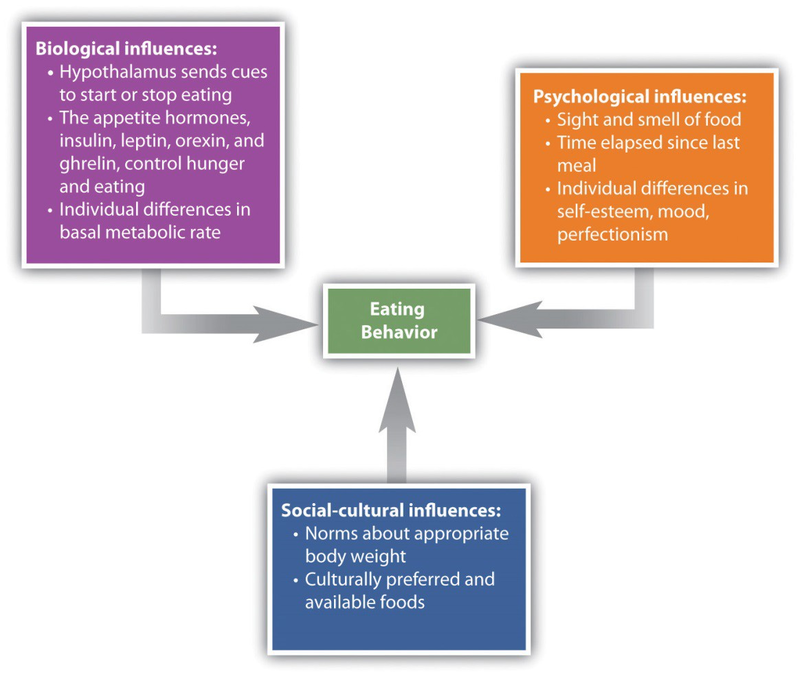
Like most interesting psychological phenomena, the simple behavior of eating has both biological and social determinants (Figure 10.9). Biologically, hunger is controlled by the interactions among complex pathways in the nervous system and a variety of hormonal and chemical systems in the brain and body. The stomach is of course important. We feel more hungry when our stomach is empty than when it is full. But we can also feel hunger even without input from the stomach. Two areas of the hypothalamus are known to be particularly important in eating. The lateral part of the hypothalamus responds primarily to cues to start eating, whereas the ventromedial part of the hypothalamus primarily responds to cues to stop eating. If the lateral part of the hypothalamus is damaged, the animal will not eat even if food is present, whereas if the ventromedial part of the hypothalamus is damaged, the animal will eat until it is obese (Wolf & Miller, 1964). 3
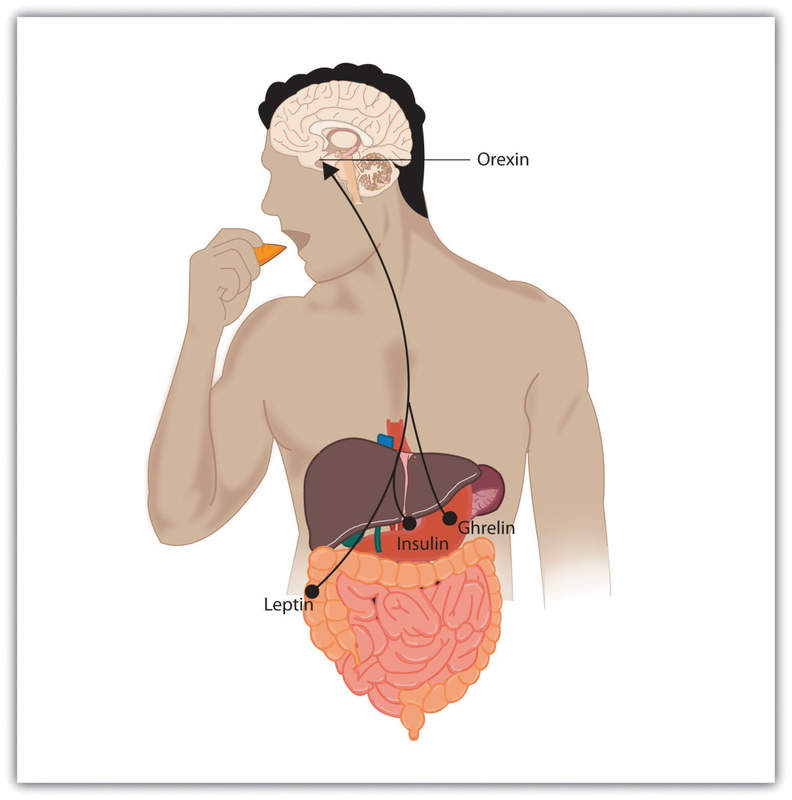
Hunger is also determined by hormone levels (Figure 10.10). Glucoseis the main sugar that the body uses for energy, and the brain monitors blood glucose levels to determine hunger. Glucose levels in the bloodstream are regulated by insulin, a hormone secreted by the pancreas gland. When insulin is low, glucose is not taken up by body cells, and the body begins to use fa t as an energy source. Eating and appetite are also influenced by other hormones, including orexin, ghrelin, andleptin(Brennan & Mantzoros, 2006; Nakazato et al., 2001). 4
Normally the interaction of the various systems that determine hunger creates a balance or homeostasis in which we eat when we are hungry and stop eating when we feel full. But homeostasis varies among people; some people simply weigh more than others, and there is little they can do to change their fundamental weight. Weight is determined in large part by thebasal metabolic rate, theamount of energyexpended whileat rest. Each person’s basal metabolic rate is different, due to his or her unique physical makeup and physical behavior. A naturally occurring low metabolic rate, which is determined entirely by genetics, makes weight management a very difficult undertaking for many people.
How we eat is also influenced by our environment. When researchers rigged clocks to move faster, people got hungrier a nd ate more, as if they thought they must be hungry again because so much time had passed since they last ate (Schachter, 1968). 5 And if we forget that we have already eaten, we are likely to eat again even if we are not actually hungry (Rozin, Dow, Moscovitch, & Rajaram, 1998). 6
Cultural norms about appropriate weights also influence eating behaviors. Current norms for women in Western societies are based on a very thin body ideal, emphasized by television and movie actresses, models, and even children’s dolls, such as the ever-popular Barbie. These norms for excessive thinness are very difficult for most women to attain: Barbie’s measurements, if translated to human proportions, would be about 36 in.-18 in.-33 in. at bust-waist-hips, measurements that are attained by less than 1 in 100,000 women (Norton, Olds, Olive, & Dank, 1996). 7] Many women idealize being thin and yet are unable to reach the standard that they prefer.
Eating Disorders
In some cases, the desire to be thin can lead to eating disorders, which are estimated to affect about 1 million males and 10 million females the United States alone (Hoek & van Hoeken, 2003; Patrick, 2002). 8Anorexia nervosais an eating disorder characterized by extremely low body weight, distorted body image, and an obsessive fear of gaining weight. Nine out of 10 sufferers are women. Anorexia begins with a severe weight loss diet and develops into a preoccupation with food and dieting.
Bulimia nervosa is an eating disorder characterized bybinge eating followed bypurging. Bulimia nervosa begins after the dieter has broken a diet and gorged. Bulimia involves repeated episodes of overeating, followed by vomiting, laxative use, fasting, or excessive exercise. It is most common in women in their late teens or early 20s, and it is often accompanied by depression and anxiety, particularly around the time of the binging. The cycle in which the person eats to feel better, but then after eating becomes concerned about weight gain and purges, repeats itself over and over again, often with major psychological and physical results.
Eating disorders are in part heritable (Klump, Burt, McGue, & Iacono, 2007), 9and it is not impossible that at least some have been selected through their evolutionary significance in coping with food shortages (Guisinger, 2008). 10 Eating disorders are also related psychological causes, including low self-esteem, perfectionism, and the perception that one’s body weight is too high (Vohs et al., 2001), 11 as well as to cultural norms about body weight and eating (Crandall, 1988). 12 Because eating disorders can create profound negative health outcomes, including death, people who suffer from them should seek treatment. This treatment is often quite effective.
- 2744 reads
